Leading Companies of the Year 2026
How Silicon Valley Revolutionized Photobiomodulation
The Silicon Review

The engineers who brought semiconductor discipline to light therapy and changed medicine in the process
Most medical breakthroughs come from inside medicine. A researcher identifies a mechanism. A lab proves efficacy. A company scales the treatment. LightMD’s story is different.
Two Silicon Valley engineers, one from semiconductors and one from computing, looked at light therapy and saw not a medical mystery, but an engineering problem waiting to be solved. The result is a company that has quietly redefined a century-old therapeutic modality. In doing so, LightMD has become one of the most credentialed, clinically adopted photobiomodulation platforms in the world.
A Century-Old Idea, Held Back by Hardware
Light therapy is not new. Its beneficial effects on human physiology have been recognized for centuries, and the field received its first major scientific validation in 1903 when the Nobel Prize in Medicine was awarded for the treatment of lupus vulgaris using light. Yet for most of the twentieth century, the technology remained a niche curiosity, limited by the only available tools of the time: hot incandescent lamps, gas discharge tubes, and large high-power surgical lasers. Burn risk, system complexity, high costs, lack of randomized medical studies, and uncertain mechanisms of action kept adoption muted.
The breakthrough that commercialized light therapy wasn’t a medical discovery, but an engineering one. The introduction of light-emitting semiconductors in 1962, specifically visible-light LEDs developed by Nick Holonyak and quantum well laser diodes by Robert Hall, opened a new frontier. Laser manufacturers moved quickly to dominate the market narrative, claiming superior penetration due to concentrated power. It was a selling point that scientific research soon dismantled, confirming that penetration depth in non-ionizing radiation is determined by wavelength, not optical power. In the 1990s, NASA embraced LED-based light therapy to accelerate healing and reduce muscle atrophy in space shuttle astronauts, lending the field its first serious institutional credibility.
In 1999, Dr. Tina Karu published a landmark IEEE paper coining the term photobiomodulation (PBM), a more precise and scientifically grounded name for what had been loosely called “low-level light therapy.” Her seminal paper established PBM as the biochemical influence of specific wavelength bands of electromagnetic radiation on cellular metabolism, identifying precise “action spectra” that drive ATP production, mRNA transcription, and protein synthesis in mitochondria. The science was compelling. The technology to reliably deliver it was not.
_2026-04-24_07-49-49.webp)
Enter Silicon Valley
Daniel Schell, a navy veteran and electrical engineer, had been studying published research on light therapy from NASA and leading universities. What he noticed was a conspicuous blind spot: while researchers focused on LED brightness and total energy delivered, the question of pulsed light was almost entirely ignored.
Schell began a methodical investigation into how varying the frequency of light pulses might affect therapeutic outcomes. The results were striking. Pulsed light not only proved more energy-efficient than continuous irradiation, it outperformed it therapeutically. More significantly, pulsing demonstrated frequency-dependent tissue-specificity: different pulse rates appeared to target different organs and physiological systems. This suggested an entirely new dimension of therapeutic control that the field had not yet considered.
Schell pressed forward empirically, building evidence-based therapeutic protocols across a surprisingly broad range of indications including pain, inflammation, wound healing, circulation, and immune function. But his research had outpaced the hardware. Most PBM systems of the era could not reliably control brightness, ensure light uniformity, prevent optical scattering, nor manage optical penetration depth. What the field needed was photonic engineering: the kind of precise, repeatable electronic control of light sources that no consumer-grade or early PBM device was designed to deliver.
The Missing Piece
Richard K. Williams was a Silicon Valley tech entrepreneur who had spent years as CEO and CTO of AnalogicTech (Nasdaq: AATI). Among the power semiconductor company’s most significant innovations were the first LED camera flash IC, the first white LED backlight driver for color smartphones, and dynamic LED backlighting systems for major-brand HDTVs. The company went public in 2005 and was acquired in an unsolicited buyout in 2012.
Following the acquisition, a mutual investor introduced Williams to Schell and the two immediately recognized their synergistic capabilities. Williams brought the photonic engineering expertise and semiconductor manufacturing discipline that Schell’s PBM research needed. Together, they founded two interrelated companies: LightMD Inc. of Cupertino, California, as the developer of advanced PBM medical devices and therapeutic regimens, and Applied BioPhotonics Ltd. (ABP) as its dedicated FDA-certified manufacturer.

Under the manufacturing leadership of Ken Lin, a veteran of AnalogicTech’s production operations, ABP engineered its first photonic controller, the LightMachine, repurposing manufacturing processes originally developed for computing and automotive electronics.
Building to Hospital-Grade Standards
From the outset, LightMD and ABP held themselves to hospital-grade standards that the light therapy industry had never seen before. ABP pursued USFDA and ISO-13485 certification for Design Control and Total Quality Management, earning a compliance portfolio that spans domestic and international regulatory bodies. Today that portfolio is what puts ABP devices at hospital bedsides while unqualified light therapy products remain barred.
The first commercial system combined an intuitive color touchscreen interface with circuit design methodologies insensitive to component variability, an engineering discipline borrowed directly from high-reliability semiconductor design. ABP ultimately earned approximately forty United States and international patents on the platform.
While ABP refined the photonic controller, LightMD focused on building the clinical intelligence to run on top of it. Drawing on a deep library of multi-spectral, tissue-specific PBM regimens and a growing understanding of frequency-dependent molecular and cellular mechanisms, the two companies co-developed an expanding portfolio of therapeutic protocols spanning injury, disease, and chronic health conditions. Organized into 20-minute tissue-specific treatments, the system gave clinicians the freedom to compose and deliver a virtually unlimited range of therapeutic regimens from a single platform.
Solving the Delivery Problem
Rigorous photonic control is only half the challenge. The other half is getting light into the body effectively.
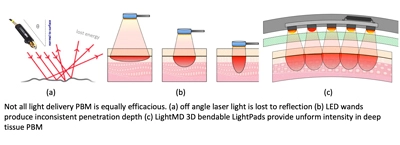
This is where most light therapy systems, including lasers, fundamentally fail. Laser-based PBM systems require a small spot size, which necessitates scanning across a treatment area. Scanning means the light beam is rarely perpendicular to the skin, and off-axis light reflects off epithelial tissue rather than penetrating it. Lasers can penetrate deeply, but only over very small areas, making them impractical for treating large muscles, visceral organs, or the brain.
Early LED systems fare no better. At just one centimeter of separation from skin, over 90% of LED-generated energy fails to penetrate beyond the epidermis. LED walls, beds, and rigid panels, the mainstay of consumer light therapy, cannot deliver meaningful energy to deep tissue. The LED must be in direct contact with the skin, and it must be perpendicular to maximize penetration.
LightMD-ABP solved this with a patented innovation they call the rigid-flex 3D LightPad, a printed circuit board that bends in three dimensions to conform to body contours without fracturing, maintaining a perpendicular angle of incidence across complex surfaces. Earlier flexible PCB designs failed because rigid LEDs would crack and detach after a few dozen bending cycles. LightMD’s engineering overcame this through novel board construction, enabling LightPads that can cover up to 1,200 cm² while delivering one Joule per cm² of red and near-infrared light directly into deep tissue, with no risk of burning the patient’s skin.
The result is hands-free whole-organ treatment at a scale no previous system could achieve. A single LightPad session can deliver deep photonic energy to large muscles, visceral organs, and through the cranium to the brain concurrently, without a therapist present. The 3D LightPad remains the only means of delivering deep tissue photobiomodulation to whole organs simultaneously.
LightMD then combined this optical delivery capability with its algorithmic PBM treatment library to release its first-generation system, the LightMachine. Clinicians responded immediately, drawn to the combination of deep, uniform optical performance and the flexibility of a hierarchical menu for selecting tissue-specific 20-minute treatments. It was a meaningful first step. But hospitals would soon reveal how much further the platform needed to go.
The Mark II: Built for Clinical Reality
The first-generation LightMachine earned strong adoption among clinicians. But hospitals exposed a new set of operational constraints that the initial design did not address. Nursing staff cannot return to a patient every twenty minutes to select a new treatment. Shift changes and handoffs create gaps in protocol delivery. And treatment menus organized around physiological parameters (such as circulation, inflammation, pain) require physicians to design their own regimens, which busy hospital doctors simply will not do.
The response was a complete platform redesign. LightMD developed LightOS, a new operating system that introduces OneTouch Sessions, predefined 45-minute sequences of red and near-infrared PBM treatments organized around specific medical conditions such as capsulitis, ankle sprain, and dyspnea. A nurse positions the LightPads, starts the session, and the patient can sleep undisturbed through the full protocol. The system eliminates both operator error and the clinical expertise burden previously required to prescribe treatment sequences.
ABP simultaneously reengineered the hardware for greater durability. The combined hardware upgrade, new operating system, and more rugged LightPads and connectors launched in 2017 as the Mark II PBM System, offered in market-specific configurations including the MedPro for physicians, ChiroPro for physical therapists, SportsPro for athletic training, DermaPro for aesthetics, and the Mark II Basic for research and general use.
The Mark II quickly became designed into clinics and hospitals worldwide, deployed across neurological, respiratory, immune, neuroendocrine, circulatory, digestive, and musculoskeletal applications. It has also been adopted by veterinary practitioners for the treatment of dogs, cats, and horses. Therapy clinics for small animals (such as PetLight.vet) provide non-surgical treatment of musculoskeletal injury, arthritis, renal dysfunction, wounds, and age-related conditions.
The COVID-19 Test
In January 2020, doctors using the Mark II began reporting an unknown viral infection, later identified as SARS-CoV-2, causing severe respiratory distress, dangerously low blood oxygen, fever, and hyperinflammation. Initial reports indicated patients with severe pulmonary dysfunction requiring tracheal intubation often ended in death.
What became known as COVID-19 rapidly escalated into a global pandemic, ultimately claiming over 7 million lives by official counts, with some estimates as high as 21 million. Doctors and hospitals were powerless. Left uncontrolled, the disease’s defining hyperinflammation triggered cascading organ failure. But suppressing it caused immunodepression, opening the door to secondary infection and sepsis. For patients with pre-existing conditions, it was a cycle that proved equally fatal.
In February 2020, LightMD convened an emergency conference call with physicians and recommended a structured PBM protocol. The protocol targeted two fronts simultaneously: disrupting viral replication while rebalancing the immune response to prevent the immunodepression that was enabling secondary infection and sepsis.
What followed was an unconventional but effective deployment. Quarantine restrictions prevented clinic visits, so doctors conducted treatments wherever possible, such as in separate vehicles in outdoor parking lots. A physician would hand patients a set of six LightPads, wrapped in plastic and connected by long cables to the Mark II controller, through a car window. The patient self-positioned the pads on their face and chest while the physician activated the session remotely. Sessions ran 45 to 60 minutes depending on severity.
The results, subsequently published in the Wiley peer-reviewed Journal of BioPhotonics, were exceptional: all 50 of the initial 50 patients recovered fully, most within three days from just two sessions and no other medical intervention. In the most severe case, acute symptoms resolved within three days, with full lung function restored after five sessions over two weeks. Expanded studies across the United States and Taiwan brought the total to 350 successfully treated patients, both outpatient and hospitalized, with no treating physicians contracting the disease.
Every Mark II model now ships with three treatment protocols born directly from the COVID-19 case studies: CNS, designed for inflammatory pain management, and epithelial protocols EP1 and EP3, developed as anti-infective PBM combatting pathogenic replication while balancing pro- and anti-inflammatory cytokines.
What’s Next
LightMD and ABP are now developing Luxy, a proprietary AI medical assistant trained to support physicians, therapists, and patients in selecting the optimal treatment and session protocols for their specific indications. It is the natural next step for a company that has always viewed medicine through the lens of systems design.
LightMD’s story is ultimately about what becomes possible when deep scientific understanding and rigorous engineering capability are built together rather than in parallel. That combination, pursued with genuine commitment to clinical outcomes, turned a promising but underperforming field into a clinical reality. And by most measures, the most significant chapters are still ahead.
LightMD Inc. is headquartered in Cupertino, California. Applied BioPhotonics Ltd. manufactures under USFDA, ISO-13485, and international regulatory certification.
Edited by Laura E. Williams

LightMD founders and Dr. Joseph Leahy, clinical researcher pioneering transcranial PBM for mTBI and brain health.